VLNC: A Bad Idea That Never Dies

In one of my, admittedly, rare perusals of the hellsite that is Twitter (I refuse to call it “X”), I stumbled across a comment from Jon Fell that caused me to stop scrolling and check the thread. The comment was:
Thank you, and that seems fair. The generational prohibition on purchase will also muddy the water when it comes to smoking prevalence for the whole population; it will be important to look at the trends for particular age cohorts too.
— Jon Fell (@JonFell73) December 14, 2022
So, what were they talking about? Well, it all stemmed from this:
Congratulations to New Zealand for passing this ground-breaking law, that includes reducing the nicotine content of all cigarettes to a minimally addictive level. https://t.co/o1IwcqZvbb
— Jonathan Foulds PhD (@JonathanFoulds) December 13, 2022
Applauding the passage of some new legislation in New Zealand which is simply an “Amendment Bill” - that is, it is legislation that amends existing legislation. Pretty standard fare for any functional legislative body - just read any of the existing Acts of Parliament from the UK and you’ll see numerous footnotes and changes. However, this isn’t a post about the legislative process.
The Bill aims to:
This bill significantly limits the number of retailers able to sell smoked tobacco products; aims to prevent young people from taking up smoking by prohibiting the sale of smoked tobacco products to anyone born on or after 1 January 2009; and aims to make smoked tobacco products less appealing and addictive.
NZ Parliament website
See, there’s similarities to the disastrous Public Health (Wales) Bill here already. Interestingly, NZ have introduced the “age escalator” for purchasing of smokes - something that even bat-shit crazy Australia has not done - yet. But, again, this isn’t the point of this post.
Y’see, they’ve opted to impose limits on the amount of nicotine in cigarettes. In the amendment bill, a whole new section (Part 3A) has now been added. For the purposes of this post, we’re going to be looking at Part 3A, Section 57H.
57H Limits on nicotine for smoked tobacco products
(1) The limit for the nicotine content in the tobacco in an individual smoked tobacco product is 0.8 mg/g.
(2) Nicotine must not be present in any other constituent of an individual smoked tobacco product, unless it is derived from the tobacco product.
Smokefree Environments and Regulated Products (Smoked Tobacco) Amendment Bill
Readers familiar with these pages will know that I have written about reducing nicotine in cigarettes a few times before, and always on the side of “that’s bloody daft” - because it really is daftness personified. But of course, there is new “evidence” that, as Foulds highlights, that show smokers don’t actually smoke more when switching to reduced nicotine products.
As vapers, we are well aware of the phenomenon known as self-titration. The act of tapering off consumption when our body decides it has had enough. It is not a conscious decision. Self-titration isn’t just limited to vaping, or smoking. In fact, a simple search on the National Library of Medicine for the phrase “self-titration” returns 722 results. It is not, by any means or definition, an unknown concept. As the Dawkins study highlighted:
Vapers engaged in compensatory puffing with lower nicotine strength liquid, doubling their consumption. Whilst compensatory puffing was sufficient to reduce craving and withdrawal discomfort, self-titration was incomplete with significantly higher plasma nicotine levels in the high condition.
So, what about this new “evidence” then?
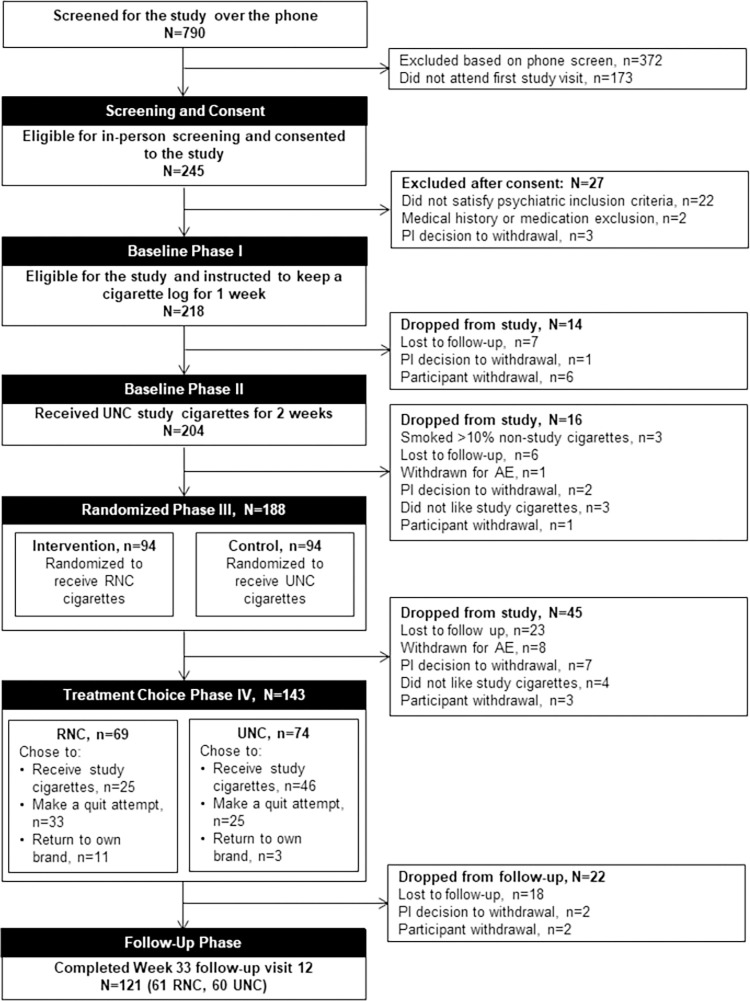
In a randomized controlled parallel group trial conducted at two sites in the USA (Penn State University, Hershey, PA and Massachusetts General Hospital, Boston, MA) 188 adult smokers with a current (n = 118) or lifetime (n = 70) anxiety or unipolar mood disorder, not planning to quit in the next 6 months, were randomly assigned (1:1) to smoke either Usual Nicotine Content (UNC) (11.6 mg nicotine/cigarette) research cigarettes, or Reduced Nicotine Content (RNC) research cigarettes where the nicotine content per cigarette was progressively reduced to 0.2 mg in five steps over 18 weeks.
Just a side-note here, using your own homework to support a policy doesn’t always end well. #JustSaying.
It is interesting that they chose smokers with a current, or lifetime, anxiety or mood disorder instead of regular, every-day smokers. Which, of course, does raise some important questions related to smoking - or nicotine consumption - and mental health in general. Not something that the referenced paper, or this post, goes in to.
At the start of the trial (Baseline I), all 188 participants smoked their usual brand for one week before being given the research cigarettes at Baseline II. From that point on, only the approved research cigarettes were to be smoked. These cigarettes were provided to the participants at no cost to the user.
Baseline II lasted for two weeks and the cigarettes provided had a nicotine content of 11.6mg.
Let’s be honest here, most people will do something if they can get free stuff or some kind of remuneration for their involvement. It is, quite simply, human nature. When we do something, we want to be rewarded for it.
Moving on to phase 3, the randomised phase. Two groups were formed (n=94), one for control (obviously) where the participants continued to smoke the 11.6 mg research cigarettes. The second received reduced nicotine content cigarettes (RNC). This phase of the trial lasted for 18 weeks and, for the RNC group, nicotine content was reduced every 3 weeks from 11.6 mg to 0.2 mg. Those in the RNC group were on the 0.2 mg cigarette for a total of 6 weeks (the last weeks of the randomised phase).
At the end of this 18-week phase, the participants were then involved in the “Treatment Choice” phase (phase 4). Participants were then given a copy of the US Surgeon General Report (which I’ve written about elsewhere) and were asked to make a choice:
1 Return to their usual brand for 12 weeks (at their own cost - an important caveat there) 2 Continue with the research cigarettes (no cost to the participant) 3 Quit smoking with counselling along with the option to use oral nicotine NRT (gum or lozenge) for 11 weeks
It is interesting to note that, out of the 143 participants that made it this far (45 were lost during phase 3), 58 chose option 3. To try and quit smoking. 14 chose to return to their own brand leaving 71 to continue with option 2. What is interesting to note here is that in the RNC group, only 25 (out of the 69 left from phase 3) chose to continue with the research cigarettes. 33 from the RNC group chose to make a quit attempt with 11 returning to their own brand.
This is illuminating as it demonstrates that, for some, reducing nicotine isn’t something they want to do. It is also known that a well-designed course of NRT (with behavioural support) that reduces nicotine content is a valid, viable way to stop smoking. It is, after all, the basis of NRT. What isn’t included in any of the supporting information with the paper is whether those participants who chose option 3 (a quit attempt) subsequently returned to smoking or managed to abstain from smoking.
So, what did they find at the end of all this? Did they, as Foulds claims in the twitter thread, NOT smoke more when switching to VLNC? Is the conclusion (“Lowering the permissible nicotine content in cigarettes to very low levels over 15 weeks reduces toxicant exposure and increases smoking cessation without worsening mental health among smokers with mood or anxiety disorders.”) correct?
Well, not entirely. (Shock, I know).
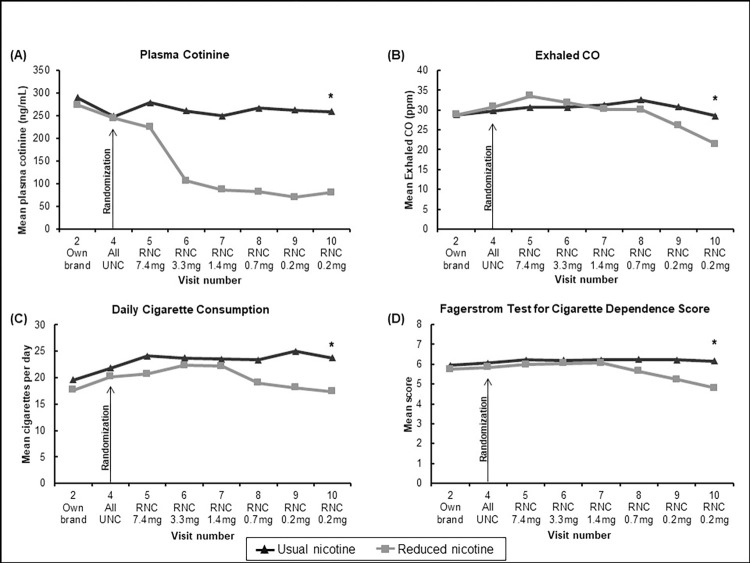
Figure 2
For the RNC group, across the 9 visits in phase 3, the mean consumption was:
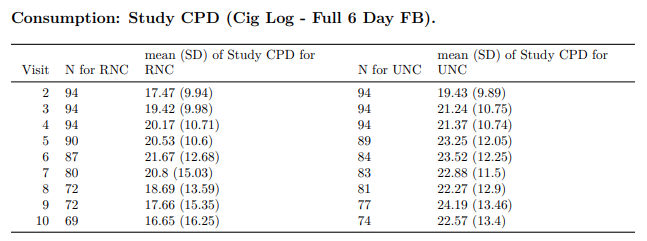
Foulds et al
Based on my own experience smoking, as I’m sure many readers can confirm, there are going to be times when you smoke more, or less and it is entirely dependent on your mood. Especially if you look at the deviations for both groups:
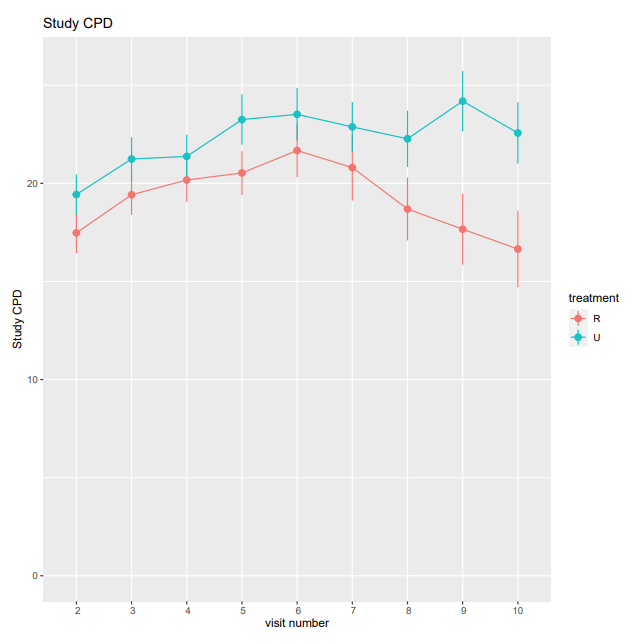
Foulds et al
Of course, the original claim (by Foulds) soon changed to “Those randomised to VLNC were about 4x more likely to quit”. Let’s look at that part of the paper:
Foulds et al
It is true that, out of the 69 RNC group participants, 33 did make a quit attempt versus the 25 out of the “regular” group (n=74). At the end of the treatment choice phase (phase 4) the study notes that 17 of the RNC group and 4 of the UNC group (“normal” cigarette strength) met the criteria for abstinence. It is worth nothing that the quit attempt was a supported attempt.
What isn’t covered in this paper is why the participants smoked. Yes, it covers the nicotine dependence aspect and after visit 7 on pretty much all tests, the RNC group did demonstrate “less dependence”, but (as with most studies of this nature), it precludes the reasoning for people to smoke. Those reasons are as varied as you can get. Not least of which many smoke because they actually enjoy smoking.
Given this paper, and the others like it, where participants are rewarded for their inclusion (both in terms of free product and financial gain as in this paper) only serve to demonstrate that, if given enough incentive, folk will do what the powers-that-be want them to.
Unfortunately, the real world doesn’t work like that. With NZ now mandating a limit on the nicotine content in individual cigarettes (just as the EU has already done), there may very well be a small uptick in the amount of smokers deciding to quit (or they may switch to alternatives) but, overall, it’ll do the grand total of diddly squat.
New Zealand, as with Australia, are now guinea pigs for state-mandated craziness and it will be a while before we can demonstrate that this policies just don’t work. It might work on some, and it is those people who are more likely to quit at some point anyway. The rest, will just have to find alternatives to enjoy because, as has been said on many occasions on this blog, it’s not about health.